Introduction:
Cardiovascular diseases are increasing worldwide including India. Diseases related to the cardiovascular system are called cardiovascular diseases. Before discussing cardiovascular diseases let us understand what the cardiovascular system is all about.
What is the Cardiovascular System?
Our body is made up of 37 trillion cells. They are grouped into tissues, organs, and systems. There are 11 systems in our body. Each system performs particular functions. The circulatory system is one of them.
The cardiovascular system, also known as the circulatory system, is a vital network responsible for transporting essential substances throughout your body. It’s like a complex highway system, ensuring that every cell receives the necessary nutrients and oxygen while removing waste products.
Key Components:
- The Heart: This muscular organ acts as the powerful pump, propelling blood through the vessels. It has four chambers: two atria (upper chambers) and two ventricles (lower chambers).
- Blood Vessels: These are the roadways of the system:
- Arteries: Carry oxygen-rich blood away from the heart to the body’s tissues.
- Veins: Return deoxygenated blood back to the heart.
- Capillaries: Tiny blood vessels that connect arteries to veins, allowing for the exchange of nutrients, oxygen, and waste products between blood and cells.
- Blood: This fluid medium carries oxygen, nutrients, hormones, and waste products throughout the body. It also contains cells that fight infection.
How it Works:
- Oxygenation: Deoxygenated blood from the body enters the right atrium of the heart. It’s then pumped to the lungs where it picks up oxygen.
- Circulation: Oxygen-rich blood returns to the left atrium of the heart and is pumped out to the body through the aorta, the largest artery.
- Nutrient Delivery: Blood travels through the arteries, branching into smaller and smaller vessels, eventually reaching the capillaries. Here, nutrients and oxygen are delivered to cells, while waste products like carbon dioxide are picked up.
- Waste Removal: Deoxygenated blood is collected by veins and returned to the heart, starting the cycle again.
The Importance of a Healthy Cardiovascular System:
A healthy cardiovascular system is essential for overall well-being. When this system malfunctions, it can lead to serious health problems like heart attacks, strokes, and heart failure.
————————————————————————————————————————–
Types of Cardiovascular Diseases
There are several arteries supplying blood to every corner of the body. If any artery is blocked, the blood supply to that particular area will be affected where that artery supplies the blood. Besides there are important organs like the heart which may also get affected.
—————————————————————————————————————————-
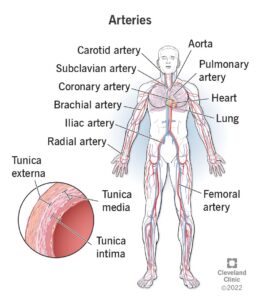
Types of Arteries
Arteries are classified based on their size and location:
- Elastic Arteries: These are the largest arteries, such as the aorta and pulmonary artery. They have a high elastin content, allowing them to withstand the high pressure of blood ejected from the heart.
- Muscular Arteries: These are medium-sized arteries that distribute blood to specific organs. They have a thicker layer of smooth muscle, enabling them to regulate blood flow.
- Arterioles: These are the smallest arteries, connecting muscular arteries to capillaries. They play a crucial role in regulating blood pressure.
——————————————————————————————————————————-
Types of Diseases
Cardiovascular diseases encompass a wide range of conditions affecting the heart and blood vessels. Some of the major types include:
- Coronary Artery Disease (CAD): This is the most common type of CVD, characterized by the narrowing or blockage of the coronary arteries that supply blood to the heart muscle. It can lead to heart attacks.
- Heart Failure: This occurs when the heart muscle is weakened and cannot pump enough blood to meet the body’s needs.
- Stroke: This happens when the blood supply to the brain is interrupted, causing brain cells to die.
- Hypertension (High Blood Pressure): Persistent high blood pressure puts extra strain on the heart and blood vessels, increasing the risk of various CVDs.
- Arrhythmias: These are abnormal heart rhythms, causing the heart to beat too fast, too slow, or irregularly.
- Aortic Aneurysm: This is a bulge or weakening in the aorta, the largest artery in the body.
- Peripheral Artery Disease (PAD): This affects the arteries in the limbs, often causing pain and cramping, especially during exercise.
——————————————————————————————————————————
Additional conditions
Here are some additional types of cardiovascular diseases that don’t necessarily involve blockages:
- Arrhythmias: These are irregular heartbeats. The heart can beat too fast (tachycardia), too slow (bradycardia), or in an irregular pattern.
- Atrial fibrillation: A common type of arrhythmia where the upper chambers of the heart (atria) beat rapidly and irregularly.
- Ventricular tachycardia: A rapid heart rate originating from the lower chambers of the heart (ventricles).
- Cardiomyopathy: This refers to diseases of the heart muscle itself. The heart muscle can become thickened, weakened, or stiff, affecting its ability to pump blood effectively.
- Hypertrophic cardiomyopathy: A condition where the heart muscle becomes abnormally thick.
- Dilated cardiomyopathy: A condition where the heart muscle becomes enlarged and weakened.
- Valvular Heart Disease: This involves problems with the heart valves, which control the flow of blood through the heart.
- Stenosis: Narrowing of a heart valve, obstructing blood flow.
- Regurgitation: Leaky heart valve, allowing blood to flow backward.
Important Note: This list is not exhaustive. Other types of cardiovascular diseases and conditions can affect the heart and blood vessels.
—————————————————————————————————————————–
Artery Blockage Locations
While blockages can occur in any artery, some common locations include:
- Coronary Arteries: Supplying blood to the heart muscle.
- Carotid Arteries: Supplying blood to the brain.
- Femoral Arteries: Supplying blood to the legs.
- Renal Arteries: Supplying blood to the kidneys.
- Mesenteric Arteries: Supplying blood to the intestines.
- Popliteal Arteries: Supplying blood to the back of the knees.
- Radial Arteries: Supplying blood to the forearm and hand.
Hence, keeping arteries clean will help us keep ourselves free from several diseases. If coronary arteries are clean we can prevent heart attack. Similarly, if carotid arteries are clean we will not have a stroke. What deposits in arteries? It is either LDL cholesterol or lipoprotein(a0 as per the latest scientific research. That means we should keep our cholesterol levels normal. Normal cholesterol levels = clean arteries = good health.
————————————————————————————————————————————-
Cardiovascular Diseases In India
Cardiovascular diseases in India are increasing due to the increase in the prevalence of CVDs and CVD risk factors. Reducing the risk factors is the strategy adopted to prevent and treat CVDs and not the underlying cause. Unless the underlying cause of CVD is targeted it seems difficult to prevent cardiovascular diseases in India like coronary heart disease and stroke.
Cardiovascular diseases (CVDs) have become the leading cause of mortality in India.
This epidemiological transition is largely because of the increase in the prevalence of CVDs and CVD risk factors in India.
In 2016, the estimated prevalence of cardiovascular diseases in India was estimated to be 54.5 million.
One in 4 deaths in India are now because of CVDs with ischemic heart disease and stroke responsible for >80% of this burden.
These diseases tend to affect patients in the most productive years of their lives and result in catastrophic social and economic consequences.
——————————————————————————————————————————-
The burden of CVD risk factors:
There are several risk factors for the rise of cardiovascular diseases in India. These cardiovascular disease risk factors are mentioned below.
Smoking:
Deaths due to smoking:
It is estimated that, currently, 275 million individuals aged >_15 years consume tobacco in India. The monthly burden attributed to tobacco in India is huge because it is estimated to cause nearly 1 million deaths annually.
Consumption of fruits and vegetables:
Indians are mainly vegetarian. It is expected that they may be eating plenty of vegetables and fruits. On the contrary, the survey shows that the rate of consumption of vegetables and fruits is low.
This is due to the high cost of fruits and vegetables. In addition, the vegetables that are consumed are often overcooked in Indian meals. This leads to the vital loss of nutrients.
Fat and carbohydrate Intake:
According to one survey, Indians’ fat intake increased from 24 to 36 g/d and from 36 to 50 g/d in rural and urban individuals, respectively.
The consumption of whole grain decreased and the consumption of refined grain products increased.
Physical activity:
Data on physical activity in India are sparse. We can say that physical inactivity is more in India.
Hypertension:
The prevalence of hypertension in adult Indians is estimated to be 30% (34% in urban areas and 28% in rural areas.).
The number of people with hypertension is expected to double from 118 million in 2000 to 2135 million by 2025.
Diabetes:
India is considered the diabetic capital. It is estimated that the number of individuals with diabetes mellitus will increase to an alarming 101 million by 2030.
Cholesterol:
Serial epidemiological studies in India suggest a rapid increase in the mean levels of total cholesterol, low-density lipoprotein cholesterol (LDL), non-high-density lipoprotein cholesterol, and triglycerides. In the ICMR-INDIAB study, a large proportion of people had at least 1 lipid abnormality. Only 20% had all lipid abnormalities (TC, LDL, HDL & TG) within the normal range. The most commonly observed abnormality was low HDL levels.
——————————————————————————————————————————–
Attempts to Prevent CVD In India
After discussing the burden of CVD risk factors, let’s examine the strategies adopted in India to prevent and treat cardiovascular diseases. These policies largely follow the recommendations of the WHO.
However, it’s important to note that many of the strategies adopted in India are based on those implemented in Western countries to combat the epidemic
Prevention and Treatment Strategies:
The strategies adopted should have been on the underlying cause of heart disease. The strategies adopted are based on reducing mortality by “reducing the risk factors”. For example, a reduction of tobacco use by a certain percentage will reduce the death rates. Similar is the case for other risk factors
Reduction of tobacco use by a certain percentage will reduce the death rates.
To the best of our knowledge, no data currently evaluates the impact of macroeconomic policy and non-personal interventions on cardiovascular disease (CVD) in India. However, modeling studies suggest that significant benefits could be achieved by imposing taxes on tobacco, palm oil, and sugar-sweetened beverages.
To combat obesity and diabetes, we propose imposing a tax on sugary beverages. Studies estimate that a 20% tax on these beverages could lead to a 3% reduction in overweight and obesity prevalence and a 2% decrease in the incidence of diabetes mellitus.
Furthermore, to reduce CVD deaths, we suggest raising the tax on palm oil purchases. Modeling studies predict that a 20% tax on palm oil could avert approximately 363,000 deaths (a 1.3% absolute reduction) from myocardial infarctions (MIs) and strokes over 10 years.
Reducing CVD deaths by a reduction in salt intake:
A moderate reduction in salt intake among middle-aged Indians, specifically a 3 gram per day reduction over 30 years, can potentially avert nearly 400,000 cardiovascular events, including heart attacks and strokes. This reduction in salt intake could also prevent an estimated 81,000 deaths, representing a 5% decrease in cardiovascular disease mortality
Smoking:
Finally, smoke-free legislation and tobacco taxation together may avert 25% of MIs and strokes in India.
Action taken by Govt. of India:
The government of India raised the excise duty on tobacco products in 2014 up to 72% and levied a new 5% tax on sugar-sweetened beverages. The moves taken are commendable.
======================================================================
Update dated 23-12-24
My Opinion on Cardiovascular Disease in India
There are two ways to look at the cardiovascular diseases in India.
Firstly the policies adopted by the Government of India depend upon what the world organizations like WHO, CDC, and American Heart Association say.
They believe in risk factors as the cause of cardiovascular diseases. So, their policies will be nothing but recommend the reduction of risk factors.
Reduction of risk factors is not the ultimate solution.
The root cause of any chronic disease boils down to cellular dysfunction micronutrient deficiency or more particularly essential nutrient deficiency. I have highlighted these points in my book Unraveling The Root Cause of Chronic Diseases. A proper understanding of the root cause is essential for preventing as well as reversing chronic diseases.
==========================================================================
Take Control of Your Health
“Tired of dealing with chronic health issues like diabetes, high cholesterol, or heart disease? Explore the underlying causes and effective strategies in my book, ‘Unraveling the Root Cause of Chronic Diseases’.”
 This is the link to BUY
This is the link to BUY
===========================================================================
The true cause of heart disease or cardiovascular diseases is the deficiency of certain essential nutrients that are essential for endothelial function and collagen synthesis. The link between Vitamin C and heart disease is well-established and documented in the scientific literature.
Tips For Cardiovascular Health
Government authorities will likely continue to focus on risk factors as the primary cause of cardiovascular diseases and other chronic illnesses. In the near future, we shouldn’t expect organizations like the WHO or AHA to significantly alter their current stance.
Ultimately, your health is your responsibility. You need to understand how nutritional deficiencies impact your well-being, as this information is often not adequately addressed by doctors. So, what should you do? I recommend purchasing my book on Amazon to enhance your knowledge of diet and nutrition.
Remember, our entire body is constructed from the food we consume, the water we drink, and the air we breathe. Every single part of our body originates from these sources. Our bodies are constantly undergoing renewal, with numerous cells dying and being replaced daily. Consequently, it’s imperative to provide our bodies with the necessary nutrients. This is a fundamental truth for maintaining good health. You must understand these principles
—————————————————————————————————————————–
Conclusion
Nutritional supplements like Lypro-c supports heart health by helping avoid heart bypass surgery as well as prevent and reverse heart disease.

Order now: for your requirement send an email to bvkhealthcare@gmail.com
——————————————————————————————————————————-
Disclaimer:
This article is for informational purposes only and should not be considered medical advice. The information provided is not intended to diagnose, treat, cure, or prevent any disease.
Always consult with a qualified healthcare professional before making any decisions regarding your health or before starting any new supplement or treatment regimen.
Individual results may vary. Lypro-C is a dietary supplement. Use it as part of a healthy lifestyle.
This article may contain affiliate links, which means we may receive a commission if you purchase through our links.
===========================================================================
Resources
Arteries: https://my.clevelandclinic.org/health/body/22896-arteries
==================================================================
Tags
#heartdisease, #cardiovasculardiseases, #heartdiseaseininindia, #cardiovasculardiseaseinindia, #CardiovascularHealthIndia, #HeartDiseasePrevention, #CardiovascularTreatmentStrategies, #IndiaHealthAwareness, #PreventHeartDisease, #CardiovascularEducation, #HeartHealthTips, #LifestyleChangesForHeart, #IndianHealthInitiatives, #CVDPreventionInIndia, #drbalaramdhotre, #unravelingtheroot causeofchronicdiseases, #root cause, #chronicdiseases
========================================================================
About the Author
Written by Dr. Balaram Dhotre, PhD — Medicinal Chemistry (CDRI, Lucknow), with research experience across several pharmaceutical companies in India. His work focuses on explaining the nutrients the body requires, how the body uses them to function optimally, and how their deficiencies are related to chronic diseases. He is the Founder of Lypro-C and author of Unraveling The Root Cause of Chronic Diseases and Reverse Heart Disease: No Lifelong Suffering.
Click here to get your copy of:::::Reverse Heart Disease: No Lifelong Suffering on Amazon
============================================================================
My Books
===========================================================================
Links on Amazon
Unraveling The Root Cause of Chronic Diseases:
Reverse Heart Disease: No Lifelong Suffering
============================================================================